







Privileging Telehealth Providers

The Telehealth Boom
By now we're all very familiar with telehealth: the remote provision of healthcarethrough the use of telecommunications technology. In fact, it is fundamentallychanging the way patients receive healthcare and is recommended by manyorganizations, offices, and urgent care centers as the first step in receivingtreatment. Over the past decade, telehealth has grown steadily as an industry.According to Global Market Insights, the market size in 2019 was around $45billion, but it is projected to grow to more than $175 billion by 2026.
Before the coronavirus pandemic, Americans were slow to pick up on the virtualtrend. But when the pandemic hit, the use of telehealth grew exponentially, andfor good reason.
Telehealth is safer for patients, as it keeps them from going into areas that maypotentially have been contaminated, which is especially crucial for senior citizensaround the country. Seeing patients remotely also gives organizations the chanceto "see" more patients, helping them scale, and patients benefit by being able toreceive more convenient and faster care. But increased adoption of telehealthalso poses a fair share of challenges.
Telehealth Concerns
Although telehealth is brimming with benefits, there are several issues involvedwith delivering it that need attention and clarification. There's confusion aboutwhat's needed to privilege telehealth providers in terms of requirements issuedby states, Medicare, The Joint Commission and other accrediting bodies, privatepayors, and miscellaneous regulatory bodies. Then there's the issue with theneed to store, share, and maintain information on telehealth providers. And finally,there's the complexities between providers being privileged to provide in-personcare in some facilities, and telehealth in others.
But there's good news, all these hurdles can be tackled. Implementing astreamlined system that privileges, stores, manages, and shares informationseamlessly is key. It's also critical to stay updated on the regulations that governtelehealth privileging and be aware of the various credentialing options availabletoday.
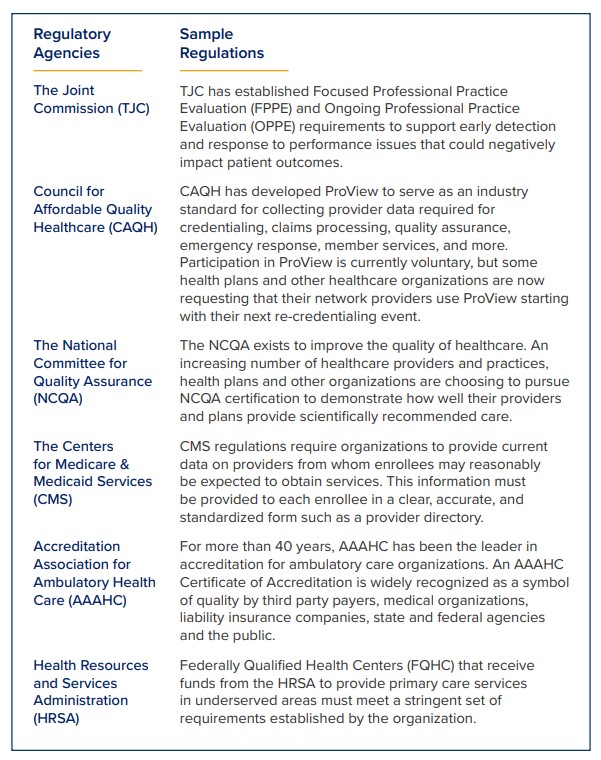
Regulations that Govern Telehealth Credentialing
First and foremost, it's important to become familiar with the different regulationssurrounding the provision of healthcare via telehealth. The Centers for Medicaidand Medicare Services (CMS) have outlined necessary requirements known asConditions of Participation (CoPs) for telehealth credentialing in detail, but hereare the basics:
- Governing Body Condition: The hospital must have an effective governing body legally responsible for the conduct of the hospital as an institution. If a hospital does not have an organized governing body, the persons legally responsible for the conduct of the hospital must carry out the functions specified in this part that pertain to the governing body.
- Medical Staff Condition: The hospital must have an organized medical staff that operates under bylaws approved by the governing body and is responsible for the quality of medical care provided to patients by the hospital.
Accredited bodies that have been awarded deemed status include:
- The Joint Commission: The new Medicare CoP requirements remove barriers to the use of telemedicine for medically necessary interventions and uphold The Joint Commission's existing practice of allowing an originating site (where the patient is located) to use the credentialing and privileging information from a distant site when making final privileging decisions for telemedicine providers.
- The DNV: Follow CMS requirements as their set standard.
With these regulations in mind, you can undertake privileging via several methods:
- Credentialing by Proxy
- Disaster Credentialing
- Traditional Credentialing
Credentialing by Proxy
Before 2011, the Medicare CoPs didn't differentiate between hospital credentialingof providers delivering in-person services versus those who provided servicessolely via telemedicine. Consequently, hospitals were required to utilize traditionalcredentialing and privileging processes for all providers, whether onsite or viatelehealth.
Responding to industry needs, CMS concluded that those regulations were servingas an obstacle to enabling widespread use of telehealth at hospitals, so a new setof regulations was designed to expedite the credentialing of telemedicine-basedproviders—Credentialing by Proxy.
Credentialing by proxy allows the hospital receiving telehealth services (knownas the "Originating Site" hospital) to rely on the privileging and credentialingdecisions made by the hospital or entity providing the telehealth services(known as the "Distant Site" hospital or "Distant Site Telemedicine Entity, orDSTE" respectively), so long as certain requirements are met.
To use credentialing by proxy, the Originating Site hospital must enter into awritten agreement with the DSTE. The agreement requires the parties to shareinformation regarding credentialing decisions, as well as periodic updates ofprovider reviews and assessments. At a minimum, periodic reports must includeall adverse events and all complaints related to each telehealth provider's servicesprovided at the originating site. Hospitals need to ensure that their process meetthese requirements:
- The distant site hospital or telehealth entity uses a credentialing or privileging program that meets or exceeds the Medicare standards that hospitals have traditionally been required to use.
- Individual providers seeking to provide and/or providing services via telehealth to the originating site have been privileged at the distant site hospital or telemedicine entity.
- Distant site hospital or telemedicine entity provides the originating site with a list of the current approved privileges for the telehealth providers seeking and/or exercising privileges at the originating site.
- Individual providers seeking and/or providing telehealth services at the originating site are licensed or otherwise authorized to practice in the state where the originating site is located.
- Originating site periodically reviews the services provided to its patients by the telehealth providers and reports this information to the distant site hospital or telehealth entity for use in performance evaluations.
- For contracts with distant site telehealth entities only, the agreement must also state that the DSTE is a contractor of services to the originating site which furnishes contracted telehealth services in a manner that permits the originating site to comply with all applicable CoPs.
These requirements are rooted in federal regulations (CoPs), but that's not all.Hospitals must also be cognizant of state laws regarding peer review decisions,confidentiality, and provider disciplinary actions, in addition to professional reviewactivities under the federal Health Care Quality Improvement Act. It's importantto note that though an organization may enter into a credentialing by proxyagreement, it retains the option to use the traditional credentialing process ifpreferred.
The key takeaway lies in the sheer potential that credentialing by proxy canoffer. If adopted at your organization, credentialing by proxy can dramaticallyincrease the speed and efficiency with which your MSO can facilitate credentialingand privileging of remote providers, saving both time and money, and moreimportantly, providing expanded care to patients.
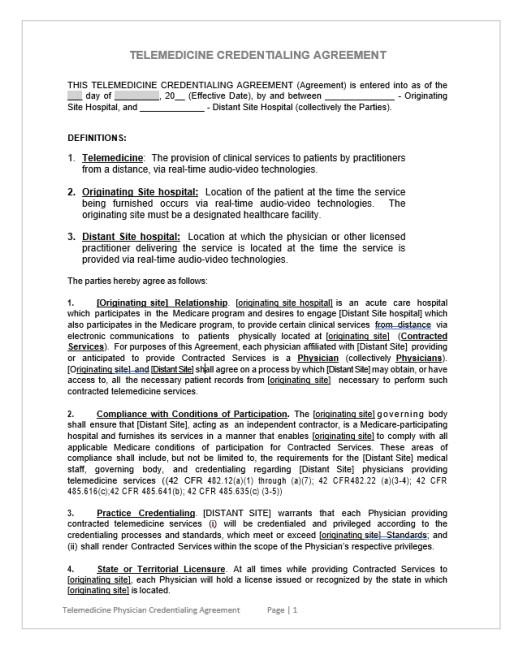
Sample of a Credentialing by Proxy Agreement:
According to the American Hospital Association,"Health systems, hospitalsand PAC providers must comply with 629 discrete regulatory requirementsacross nine domains."
Disaster Credentialing
According to The Joint Commission, a disaster is an emergency that due to itscomplexity, scope, or duration, threatens the organization's capabilities andrequires outside assistance to sustain patient care, safety, or security functions.Because disasters often mean uncertainty, The Joint Commission Standards statesthat during disasters, hospitals may grant disaster privileges to licensed volunteerindependent providers. The standards for this are pretty simple, it requires that themedical staff bylaws of the organization include a process for approving providersfor the care of patients in the event of an emergency or disaster. Once a disasterhas been declared, there are a couple of steps that must be taken.
- Verify provider identity with a government-issued ID, such as a driver's license or passport
- Verify licensure within the state—in some cases, states have waived the need to be verified in the same state, so it is up to the organization to follow their state's protocols
And that's it, your organization will be ready to go! This expedited disastercredentialing procedure is a sure-fire way to fulfill requirements easily so that youcan begin to offer expanded patient care quickly. If your health system is going toneed to grant telehealth privileges to providers who are not part of your system,disaster privileging is the way to go.
Traditional Credentialing
If Credentialing by Proxy or Disaster Credentialing isn't a fit for your needs, youcan always follow a traditional credentialing process if preferred. In that case, it'simportant to keep in mind that all accrediting organizations require:
- That you have a governing body in place that is responsible for all privileging decisions.
- That you have clearly defined credentialing and privileging policies and procedures that identify:
- The scope of the care your organization is providing www.veritystream.com
- Who is required to be credentialed and/or privileged to deliver those services
- The qualifications that a provider must possess to be privileged to practice those services in your facility, such as education, training, experience, board certification, etc.
- A process for verifying the qualifications required
- A process for making privileging decisions (Credentials Committee or other authorization pathway)
Managing Telehealth Providers Within a Health System
Credentialing may be slightly different within a health system. A health systemwill often have providers who are fully credentialed and privileged at somefacilities within the system, but then only provide telehealth services at others.If the privilege delineations at the facility where the provider has full privileges(distant site) are written comprehensively, the provider would not need tobe granted separate privileges to authorize the telehealth services they areproviding (to the originating sites), as they would already be inclusive in theirfull privileges. This is because it's common practice for health systems to utilizethe same credentialing and privileging solution, which makes it easy to shareinformation between sites.
Telehealth is Here to Stay
AAs 2020 continues to challenge us, the need for telehealth will only grow andquickly become the norm. That's why implementing a first-rate privileging andcredentialing system designed to work on the cloud is of the utmost importance. Ifyou're not certain about your organization's ability to perform proper credentialingand privileging, be it for telehealth or in-office providers, now is the time to act.Implementing an automated system that is comprehensive, scalable, and effectiveis easier than you think, and better yet, VerityStream will ensure everything goesaccording to plan.
With CredentialStream you can leverage technology to increase patient volumeand satisfaction.
With automated procedures, you will set your organization up to deliver withspeed, consistency, and certainty. CredentialStream has everything yourorganization needs to request, gather, and validate information about a provider.With a continuously updated platform, best-practice content libraries, and industryleading data sets, CredentialStream is the most comprehensive provider lifecycle management solution available. Most importantly, the solution is built to grow with your organization; based on your needs you can add functionality to assist with credentialing, privileging, enrollment, onboarding, evaluation, and networkmanagement.