







What Medical Services Professionals (MSPs) Should Know About Life Support Certification

Organizations typically either require all providers to have some type of basic oradvanced life support or they require some specialties to maintain certification.This paper has been written to provide education to Medical ServicesProfessionals about the providers of basic and advanced life support, howcriteria should be written and other issues that are relevant and important for anorganization to consider when establishing their internal standards.
The Use of Criteria in Privileging
During the early years of privileging (1970s and early to mid-1980s), privilegingcriteria was scarce - almost non-existent. Privileges were laundry lists and therewasn't a lot of emphasis on confirmation of current clinical competency prior togranting privileges. Typical criteria included items that we would consider todayto be more related to membership criteria - such as living within a certain distancefrom the hospital, having malpractice insurance, etc. When privileging criteriabegan to be incorporated into privileging decisions by healthcare organizations, itwas typically because something new had been introduced - some type of deviceor new methods of performing procedures.
Privileging criteria became much morewidely used beginning in the early1990s due to the impact of the NationalPractitioner Data Bank when it becameunderstood that an organization didn'thave to deny a provider a privilegeif the provider didn't meet the statedthreshold eligibility requirements forthe privilege. This was advantageousto both the provider (because he/shewouldn't have a denial of privilegeson his/her record and a report tothe NPDB) and for the organization(because there is no report to theNPDB, there is no requirement for ahearing).
As criteria became more widely implemented, it also moved from separatepolicies and procedures to being defined on the privilege delineation itself. Thereason for this, of course, is that organizations want the criteria to be clearly visibleto applicants for privileges as well as to those who recommend privileges.
Today, criteria is fundamental to the privileging process because the Centers forMedicare and Medicaid Services (CMS) are extremely direct in their requirementsthat privileging be criteria-based (and CMS requirements drive the standards ofthe accrediting organizations, such as The Joint Commission, that have "deemedstatus" with CMS).
The following is an excerpt from a November 12, 2004 letter (the completedocument is attached to this document) from the CMS directed to State SurveyAgency Directors related to how privileging must be surveyed.
The hospital must have a privileging process in place that complies with CMSrequirements. The hospital's privileging process must be in compliance withthe hospital CoPs at §482.12 (Governing Body), §482.22 (Medical Staff), andwith other CoPs that require medical staff oversight of practitioner qualificationsand privileges, federal and state law, and the process must be approved by thehospital's Governing Body. The hospital's Medical Staff bylaws must describe theprivileging process to be used in the hospital. The process must include criteriafor determining the privileges that may be granted to individual practitioners and aprocedure for applying the criteria to individual practitioners.
We recommend that privileging criteria be clear and concise - and mostimportantly, be consistently applied. And we must always remember that the goalof privileging is to assure that only providers who can demonstrate competencyare granted clinical privileges - thus providing benefit and protection to patients.
As we explore requirements related to certification for basic and advanced lifesupport, we must remember that certification is criteria that relates to the exerciseof specific privileges. It is not a privilege by itself or that stands alone. Below isan example of "what not to privilege".
Don't Do This
Certifications for Basic, Advanced Life Support and PediatricAdvanced Life Support (BLS, ALS and PALS)
Looking Back at Requirements for Life Support Certification
Many medical staff organizations in the past required basic or advanced lifesupport as a requirement of medical staff membership or as a requirement forany type of clinical privileges. The reason for requiring certification was to assurea basic level of competency for all providers (including nursing) to identify andreverse a cardiac or respiratory arrest (basic life support) or to support the patient(advanced life support). In the 1980's, when many hospitals implemented CodeTeams, it was important to identify what providers could lead the team as wellas those who could serve as a team member. And - at that time, because ofthe variations in training in residency programs, it could not be assumed that theskills to lead a team were always incorporated into residency training programs.Therefore, certification in basic and/or advanced life support was a credential thatbecame vital to many healthcare providers and hospitals.
If basic or advanced life support was a membership requirement, it was includedin the medical staff bylaws and listed with other membership requirements. Ifit was a basic requirement for clinical privileges, it was included in the bylawsarticle related to clinical privileges. Or sometimes the requirement was listedin the medical staff rules and regulations. In many cases, the requirement waswritten as "basic" or "advanced life support certification" from the American HeartAssociation (AHA). And, as often occurs with these types of documents, they donot get changed until it becomes apparent that an update needs to be made, asis occurring today because of another option for training and certification - theAmerican Red Cross (ARC).
Facts Related to BLS, ALS and PALS
- The International Liaison Committee on Resuscitation (ILCOR) is the organization that sets international guidelines for resuscitation. ILCOR's evidence evaluation is undertaken and lead by ILCOR's member organizations and other evidence based national and international leaders in resuscitation such as the American Red Cross and the International Federation of Red Cross and Red Crescent Scotties (IFRC). These guidelines are referred to as CoSTR (Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations). ILCOR was formed in 1992 as a not-for-profit organization to develop and disseminate international consensus statements or guidelines for resuscitation. National organizations who provide evidence based training such as the American Red Cross and the American Heart Association take the ILCOR CoSTR and adapt them as appropriate to their regions. For example, some 23% of deliveries in The Netherlands occur at home, and The European Resuscitation Council standards reflect this divergence from the international norm. In the past while both the ARC and AHA took the ILCOR guidelines and adapted them to the US, the AHA was the only organization to offer ALS and PALS. That is why when discussing ALS and PALS, many refer to the guidelines as being from the AHA when in fact the origin of guidelines is ILCOR, which are then the basis for both the ARC and AHA programs.
- Training and certification from the American Red Cross and the American Heart Association are based on the same evidence reviewed and treatment recommendations developed through the ILCOR process. Both offer classroom training with a certified instructor or online blended with a feedback manikin.
Recommendations Related to Credentialing and Privileging
1. Do not specify a specific provider of training/certification in bylaws, policies andprivileging criteria.
Organizations have, in their quest to be specific, identified one provider intheir documents, for example: "Current certification in ACLS from the AHA."This therefore eliminates the possibility for healthcare professionals to seekcertification from educational providers who offer equivalent and in the view ofsome students and organizations preferred programs such as that offered by theAmerican Red Cross. See #4 (below) for the way that criteria should be written.
2. Determine what healthcare providers must maintain certification.
It is up to each organization to determine the extent to which certification mustbe maintained by healthcare providers. Some organizations want all healthcareprofessionals (nursing and physicians) to maintain life support certification -others will make their requirements specific related to the privileges held byproviders/
Medical staff bylaws, rules and regulations or policies should state either that BLS,ALS or PALS certification is required for all privileged providers (based upon theirpatient care responsibilities) OR that requirements related to certification for basic,advanced life support or pediatric advanced life support will be specified withinapplicable privilege delineations.
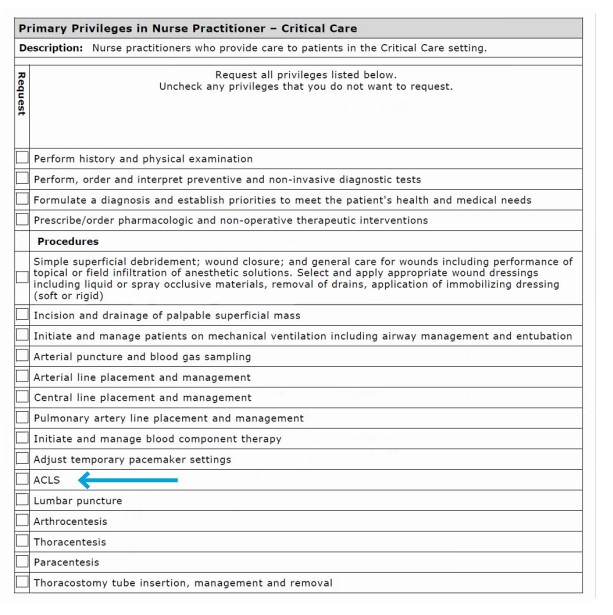
Appropriate Method of Documenting Criteria on aPrivilege Delineation (s for a Nurse Practitioner-Critical Care)
3. Specify the type of trainingthat qualifies.Providers of training/certification must providetraining and certificationbased on ILCOR guidelines.Additionally, skills validation isrequired to be a componentof the curriculum (i.e., thecertification cannot bebased on training exclusivelyobtained online).
4. If life support requirementsare related to specialties,determine the privilegingcriteria and the specialties to which the criteria is applicable.
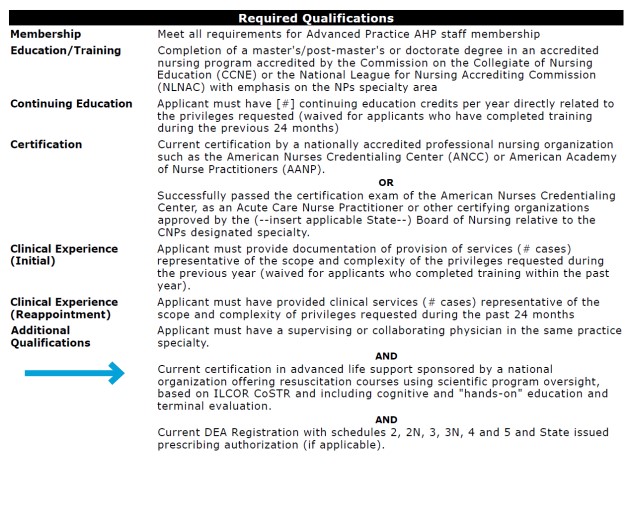
Privileging criteria should be written to be unambiguous. Here is an example:"Current certification in (insert type of certification that is required - i.e., ALS,PALS) sponsored by a national organization offering resuscitation courses usingscientific program oversight, based on ILCOR CoSTR and including cognitive and"hands-on" education and terminal evaluation."
5. Determine timeframes for validation of certification.
Consider pros and cons when options for verification timeframes are selected.The options include:
Initial credentialing: Verification of current certification as required.k At expiration or renewal of privileges:( At expiration of the credential( Verify currency at renewal of applicable privileges (i.e., every two years)
Determination of the appropriate option should consider the following: Is itmore important to target your management systems to enforcing expiration? Oris it more important that the privilege holder review and update their skills andrecertify every two years? If the applicable certification is updated at the timeof recredentialing, there is plenty of advance notice of the pending renewal ofprivileges and the requirements that must be met at that time - and it is less likelythat there will be lapses in privileging due to expiration of life support certification.
If your organization determines that it is appropriate to update every two years(rather than at expiration) your privileging criteria might state: "Current certificationin (insert type of certification that is required - i.e., ALS, PALS) sponsored by anational organization offering resuscitation courses using scientific programoversight, based on ILCOR CoSTR and including cognitive and "hands-on"education and terminal evaluation. Evidence of current certification is required atinitial appointment and at the time of reappointment."
6. Other considerations.
Organizations may want to provide their providers with an incentive to use aspecific training and certifying organization in order to facilitate compliancewith their internal requirements and to make it convenient for their healthcareproviders to achieve certification. Selection of a provider of education andcertification with the capacity to provide classes/programs that are readilyavailable is essential.
At VerityStream we are proud to offer our employees and organizations trainingprovided via the American Red Cross. The American Red Cross program isthe most innovative resuscitation program in the world, leveraging the latesttechnologies for manikin, simulation, virtual reality, adaptive learning and more.
The ARC uses an adaptive learning model that saves individuals and organizationssignificant time. Healthcare providers that can demonstrate competence up-front,do not have to go through all of the course materials. For on-the-go learners, thecontent works with smartphones, tablets, and laptops.

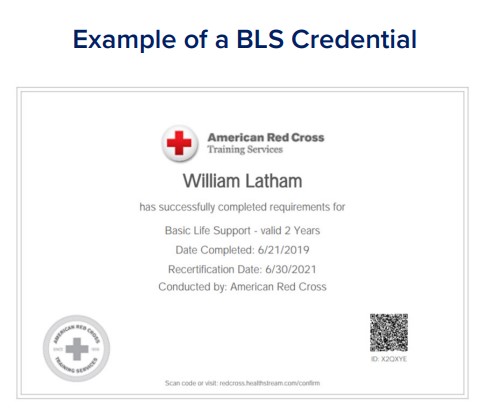
If your organization has a direct link into yourprovider/credentialing software that providesdynamic verification of basic or advanced lifesupport from the certifying organization -your job of tracking this information is madeexponentially easier! The Red Cross andHealthstream partnership allows this type ofdynamic primary source verification. It alsoprovides you a validated credential in BasicLife Support, Advanced Life Support andPediatric Advanced Life Support.
Finally - let's remember why life supportcertification is important:
When every member of the resuscitation team is both competent and confident,lives are saved.